

- An Amazonian ant whose venom is considered one of the most painful in the world. Hence its nickname of "bullet ant", as its sting is said to resemble the effect of a bullet wound. Don't ask us how we know that.
- Or not so little.
- It was Galenus, in particular, who discovered the renal origin of bladder stones by poking around in dead animals. And in some gladiators. Also dead, and quite often pre-chopped.
The fear of bladder stones
Which pain was worse? A renal colic or the removal of urinary calculus? Whoever did it needed to master the technique and understand the patient.
In our Medical History articles, author Jean-Christophe Piot describes the most significant stages in the history of medicine with a lot of research rigour and a bit of humour.
Translated from the original French version.
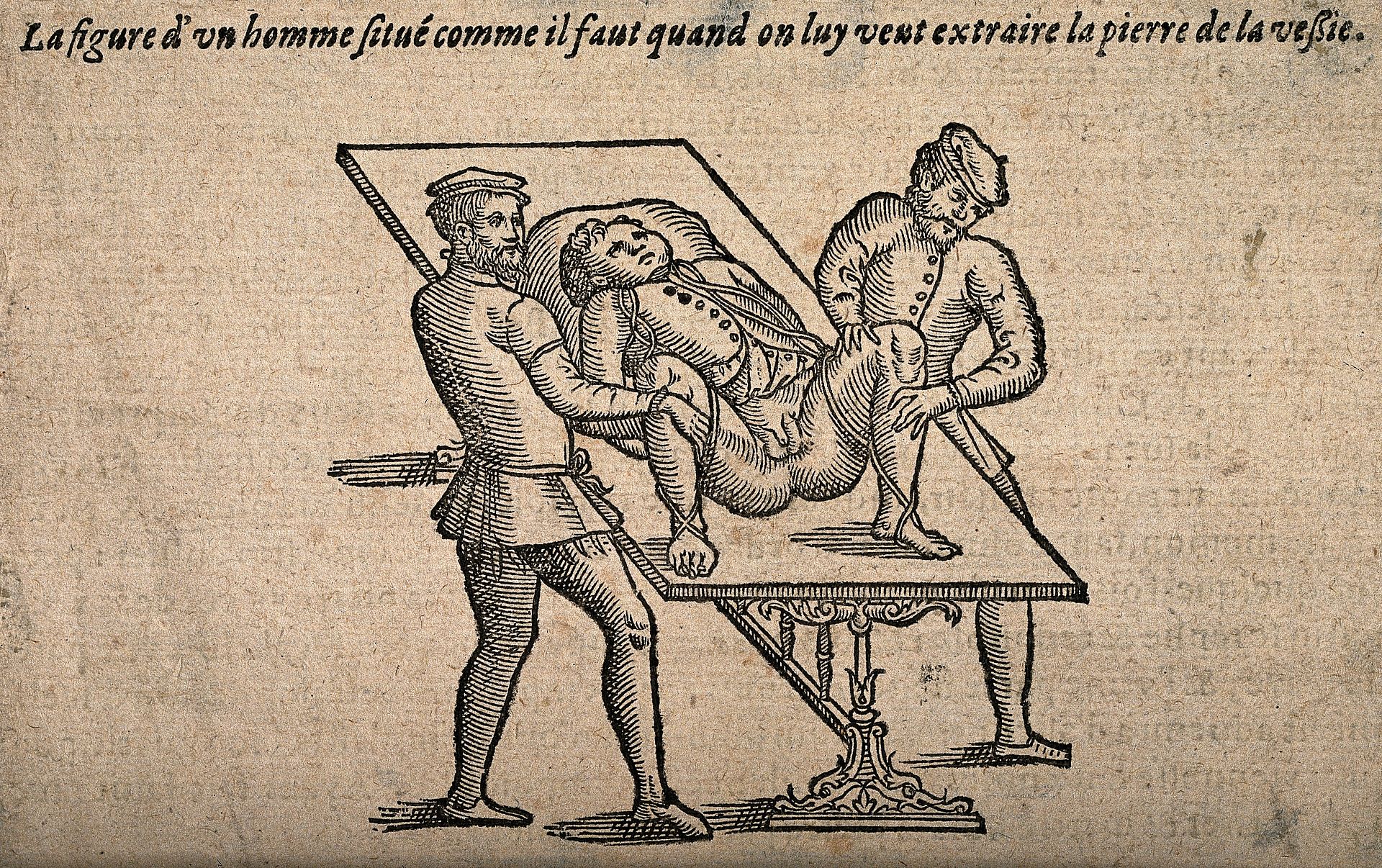
"A very calm patient. The illustration may not depict expressions accurately."
In the ranking of pains you wouldn't wish upon anyone, renal colics rank just a step behind toothaches and a mere whiff away from the bite of a Paraponera1. Though, the unlucky patients of the 21st century can count on the advancement of medicine to provide them with quick relief and treatment. This is a privilege, considering that, until the 19th century, people tended to dwelve in the pain until a doctor came along. And the best was yet to come, when those little2 concretions were to be dislodged... Here´s an overview of how Hippocrates' disciples have fared over the centuries on this problem.
As Alexandre Vialatte could have said, kidney stones date back to ancient times. Archaeologists regularly find them and one of the oldest cases involves an Egyptian mummy discovered in 1901, a good seven thousand years after the mummy's death in 5000 BC. In contrast, while a few papyri have been found that suggest herbal treatments, there is no record of any surgical treatment prior to classical Greece.
The original text of the famous Hippocrates oath expressly states this in the 4th century: "I will not perform the operation on the waist, I will leave it to the people responsible for it". From this we can draw some conclusions: Stone-cutting was a matter for specialists. It consisted either of extracting stones with a small bronze curette or of cutting or crushing any stones that were too large to be extracted with a hook inserted into the bladder. And it was a risky business. It wasn’t until two centuries after Hippocrates that a doctor from Alexandria broke his oath, and he is remembered as Ammonius the Lithotomist.
The famous bronze curette. To be inserted... you know where
The first rule of surgery: cover your ears
As for a precise description of the surgery, we have to wait until the time of Augustus of Rome. We find it in the De Arte Medica written by Celsus, the first practitioner to provide a precise protocol for the incision operation, of which he wasn’t aware of neither the risks nor the possible complications. From haemorrhage to gangrene, they are so severe that he insisted it should only be attempted when all else had failed, starting with the insertion of fine brass probes into the urethra.
In the event of a failed operation, good luck to the patient: The procedure is performed, of course, without anaesthesia, and involves a rectal palpation intended to "push" the stone found by said touch towards the surface of the body, before proceeding with the other hand to make an incision in the perineum, the prostate and the bladder neck in order to extract the stone with a hook. All of this is accompanied by a great deal of screaming, as one can imagine. Celsus acknowledges that a successful surgeon must "be able to use both left and right hands, have excellent eyesight, and act with courage and determination without wavering in order to heal the patient despite his cries."
The technique of Celsus, refined by the other great physician of the Roman Empire, Galenus3, was to remain the de facto standard of medical practice throughout the late Roman period and well into the Middle Ages. And even then, one can consider oneself fortunate if the ancient knowledge had been preserved in a nearby monastery and studied by the local physicians, who were generally... well, the monks themselves. As for the poor sick person who complains a little too much, he risks being comforted by a priest who will encourage him to remember that pain brings him closer to the sufferings endured by Christ. A therapeutic approach that has its limits.
The patient is "properly positioned". A reassuring situation...it is not
During the Renaissance, even Ambrose was not that much of a Paré
From the 15th century on, Europe entered a phase of profound cultural progress, largely based on the rediscovery of ancient texts. In medicine, as elsewhere, the renaissance allowed for the rediscovery of previously buried knowledge, and then to push it further, with the first advances in anatomical science. Now, things were still fairly traditional. One famous and knowledgeable patient, Montaigne, stuck to the humoral theory to explain the bladder stones from which he suffered from the age of 40. The author of the Essays hid nothing about his sufferings: “The obstinacy of my stones, especially in the penis, has sometimes thrown me into long periods of suppressing urination of three, four days: And so close to death that it would have been madness to hope to avoid it, or even to desire it, given the cruel efforts that this state brings me (…) They see me sweating, turning pale, blushing, trembling, vomiting till I bleed, suffering strange contractions and convulsions, sometimes dripping big tears from my eyes, emitting thick, black and horrible urine, or else having it stopped by some thorny, bristly stone which punctures you and cruelly scratches the shaft of your penis...” (Essays, III,4 et III,13).
In short, he held on to the stones, especially since few people dared to operate. Even a surgeon as gifted as Ambroise Paré was still cautious and would rather have avoided operating as much as possible, preferring a gentle extraction when the stone is no longer in the bladder: “Once the stone has come out of it or remained in the shaft or penis, the surgeon must be careful not to push it back in. Instead, he must push it out as far as possible with his fingers from the root of the penis, putting in sweet almond oil or other lubricating substances. And if it comes down to the tip of the penis and remains there, it must be pulled out with small hooks. And if it cannot be extracted with such hooks, we shall put this instrument called an anchor screw with its cannula into the penis right up to the stone. Then it will be rotated gently to break up the stone into small pieces...”
Stings a little? It is even better when it comes to surgery. If this technique fails, Ambroise Paré has a solution which will leave you dreaming. Frankly, you can't help it, it's too good: “In case [the stone] is so large or has so many rough edges that it cannot be pulled out, an incision must be made, which I have done several times (...) The incision must be done on the more fleshy side of the penis. But you should note here that before making that incision, you must bind the penis above and close to the stone, in order to keep it constrained, and then pull the foreskin towards you strongly enough so that after the incision the skin is relaxed and returns to cover the cut. This will allow for an easier and faster joining and healing of the wound afterwards.”
We are reminded that the good Ambroise's motto was "Hard work conquers all". Some restrictions apply
Ambroise was not the only one of his time to joyfully cut open lower bellies. Pierre Franco is another example: Settled in Lausanne in the 16th century, this Provençal-born made a name for himself throughout Europe as a "cutter of bladders, hernias and cataracts". In particular, he pioneered an innovative technique of cutting the lower urethra and inserting a metal probe, called an itinerarium, with a groove in it. This allows an instrument to be inserted to break up the stone before extracting it along with its debris. The case of Franco was not uncommon: from the 16th to the 18th century, itinerant specialists travelled throughout Europe offering their services.
They often originated in Germanic countries and had the name of Steinschneider, the stonecutter, a name still often borne by German families who are likely to count one of these practitioners among their ancestors. Specialists can also be found in the large cities, often in the hospices: For instance, Jacques Beaulieu practised from the end of the 16th to the beginning of the 17th century and was the official specialist in kidney stones for the French court. He performed the operation through sectio lateralis, meaning from the side. He was the specialist who was called in as a last resort when all else had failed, and with good reason: the chances of survival were between 30% and 50% until at least the beginning of the 18th century.
When you add to this other side effects, such as impotence or the occurrence of urinary fistulas, it is easy to understand why the surgery was associated with pure faith and considered by patients to be a quasi death sentence. Marin Marais, a disciple of Lully and the king's violist, was so impressed by this that he composed a viola da gamba piece directly inspired by the operation, intended to express the anguish of the "stoners": the Théâtre de l'Opération de la Taille, a piece that follows the procedure step by step, in a highly codified manner.
All five on the sick one
In concrete terms, and knowing that one couldn’t obviously count on anaesthesia to keep the patient still, the operation was all the more complex as the cut was simple. In the 16th century, the "small apparatus" was gradually replaced by the "large apparatus", which required the use of a whole range of increasingly sophisticated instruments.
For the small apparatus, two servants were sufficient. One big man who took the patient on his knees and forcibly spread both arms to keep him still, another one whose job was essentially to lift the patient's testicles so that the surgeon saw without obstacles. For the large apparatus and the sideways cut, things got technical. A tilted surface was set up, often a simple table wedged against a mattress. The patient was then placed on the edge of the table and his arms, thighs and legs were tied. Three assistants were brought in to keep the patient still, while a fourth was responsible for pulling up the scrotum and holding the catheter. A fifth man acted as an auxiliary, handing the surgeon the instruments he needed. The operation itself took only a few minutes if all went well.
And if it didn’t? According to a witness of the time, this is what happened: “The stone escaped the pliers several times; several pliers were broken; several surgeons were exhausted. One spectator said that the unfortunate patient's prayer should be heard, as he begged to be left alone and put back in his bed (...) but the surgeon did not want to abandon either the table or the victim. (...) Finally, the patient was exhausted and could only utter faint cries (...) when, after two hours of horrible suffering, they agreed to untie him and put him back in his bed, where he died about an hour later.”
Little by little, however, medical progress gave patients better chances. Anaesthetics and antiseptics were introduced and above all allowed pain to be reduced, thanks to ether, which was used more commonly in the mid-19th century. Surgical techniques became more precise with the emergence of endo-urethral lithotripsy, which became established after 1835, while urology developed as a speciality in its own right.
That said, we can't resist inviting you to take a look at what is probably one of the rare screen representations of such an operation, taken from the series Deadwood, which is set in the American Black Hills (South Dakota and Wyoming, USA) around 1870. As you can see for yourself, the very well documented series shows that anaesthetics were not among the most common commodities in South Dakota.